Improve Mitochondrial Function & Reduce Oxidative Stress
Omaveloxolone (Brand Name: SKYCLARYS for >16yo)
Biogen
Learn moreAvailable to patients >16yo; Phase III <16yo
Available to patients >16yo; Phase III <16yo
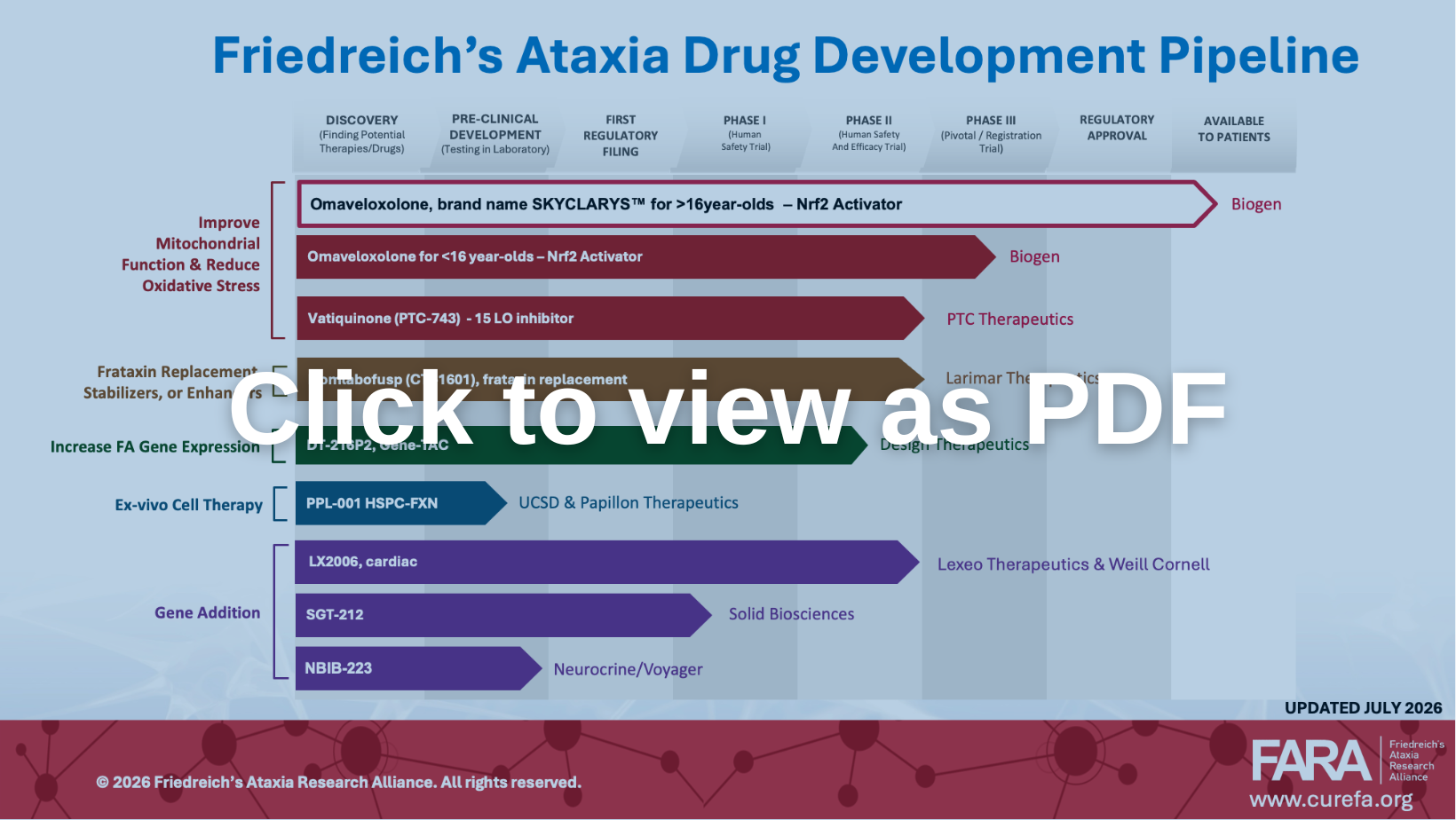
Improve Mitochondrial Function & Reduce Oxidative Stress
Biogen
Learn moreImprove Mitochondrial Function & Reduce Oxidative Stress
PTC Therapeutics
Learn moreFrataxin Replacement, Stabilizers, or Enhancers
Larimar Therapeutics
Learn moreGene Addition
Neurocrine Biosciences / Voyager Therapeutics
Learn moreInactive
Berta Alemany, Institut d’Inverstigacio Biomedica de Girona
Learn moreInactive
Children’s Hospital of Philadelphia
Learn moreInactive
Department of Neurology, Innsbruck Medical University, Innsbruck, Austria; Federico II University
Learn moreInactive
Richard Festenstein, Imperial College; Jorg Schulz, Aachen University
Learn more